
Living with invisible disability
When we think about disability, we usually picture someone in a wheelchair or with a guide dog. However, 90% of the 4.4 million people with disability in Australia are living with invisible disability. An invisible disability is a disability that you cannot see. Sometimes it can be easy to see someone’s disability, for example if they use a cane, or a hearing aid, but sometimes disability isn’t visible.
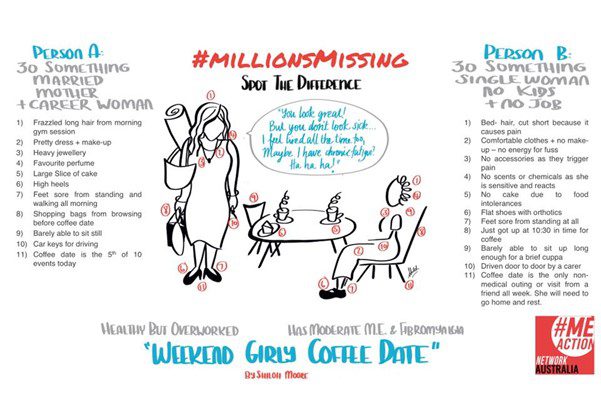
QDN member Erica Eele is one of those people. We recently spoke with Erica to talk about her experience of invisible disability, including chronic illness, and how it has affected her life. Erica has worked in marketing in the IT industry and in senior policy roles and loves cats and easy cycling. Erica also has myalgic encephalomyelitis (ME), also known as chronic fatigue syndrome. Myalgic encephalomyelitis is a complex acquired neurological disease with numerous symptoms related mainly to the dysfunction of the brain, gastro-intestinal, immune, endocrine, cardiac and circulatory systems.[1] [2] [3] Erica's ME was triggered by getting food poisoning and then catching the flu, resulting in a sudden onset of the disease.
Living with an invisible disability like ME can be challenging, with many of ME’s fifty-plus symptoms [4] not well recognised. During her more acute phase of ME, Erica’s energy impairment meant even sitting upright for a few minutes would result in full body pain and drain almost all her energy for hours or even days. Since she could barely whisper and could only hold or look at a mobile screen for about twenty seconds, Erica became isolated. She recalls gazing at a bird in her tiny courtyard to feel a sense of connection to the outside world. Despite being highly fit and active before ME, Erica became one of the estimated ‘invisible’ 600,000 Australian residents who are homebound or bedbound. [5]
While her energy levels and other symptoms have recently improved, Erica still has hyperacusis, which means she is extremely sensitive to sound.
“Sometimes even minor sound, such as someone saying, ‘gidday!’ can feel like being slightly ‘electrocuted’, explains Erica.
“Just the sound of two people talking can trigger all of my symptoms, which can make it really difficult to participate in group conversations.”
“Going out in loud public places, going to the doctor, or doing grocery shopping in person can be very challenging, even when I wear my customised ear plugs.”
Erica will often attend events or appointments remotely. If this is not an option, she asks if she can wait or sit separately, otherwise she may not be able to participate. Despite this, Erica says she is one of the more high-functioning members of the ME community, with 25% of over 500,000 of her ME peers in Australia home-bound or bed-bound.
Erica believes that disability should not be defined solely by visibility and feels she doesn’t meet the socially constructed expectations of what it means to have a disability.
“Every time I park in a disability parking bay, I worry about being abused,” says Erica.
“It goes back to the assumption of what constitutes disability; that it must be visible, non-fluctuating and constant.”
According to a UK study on over 70 energy-limiting chronic illnesses, people with ELCIs, ‘fatigue’ was identified as the most debilitating yet most socially disbelieved and dismissed symptom. [6]
Erica says one of the challenges for people with energy impairment is that the language suggests people are ‘just a bit tired’, but many people are literally bed bound for decades.
“Many of my family and friends don’t know much about it, they’re politely quiet and bewildered and accept what I say,” says Erica.
“Some people, even some of my own family members, say it’s all in my head.”
“Before I was diagnosed, I was a bushwalking and cycling trip leader and accessibility rarely crossed my mind, but here I am.”
Erica says that the severity of symptoms, the availability of treatment, attitudes towards disability, the prevalence of the condition, and social environmental factors are all important considerations.
“My view is everyone has various levels of function,” explains Erica.
“It is important that low-functioning conditions are considered as disabilities.”
Erica’s advice for others is to:
- Speak even if your voice shakes, because if you don’t speak up, who will?
- Start small to build confidence and be patient.
- Connect with others – you can’t do it alone. Connect with peers for support and inspiration, look to other communities.
- Use concrete examples in describing one’s symptoms. For example, instead of, “I have limited energy”, “My limited energy means I can only sit up for 5 minutes.”
- Pick your battles. Not everyone will understand or accept.
- In advocacy, while human rights-based rationales are important, emphasising economic reasons will more likely sway decision-makers.
[1] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4878662/
[2] https://www.nhmrc.gov.au/me-cfs
[3] https://mecfs.org.au/about-mecfs/
[4] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4878662/
[5] https://figshare.com/articles/online_resource/Making_the_Invisible_Visible_Exploring_the_Experiences_of_Frail_Homebound_and_Bedridden_People/14417987/3
[6] https://chronicillnessinclusion.org.uk/wp-content/uploads/2021/04/energy-impairment-and-disability-inclusion.pdf